
Ear, Nose, and Throat

Pregnancy affects almost every aspect of the ear, nose, and throat – symptoms of which can be pretty intolerable.
These symptoms are almost solely the result of the dramatic increase in blood volume that starts very early in pregnancy and impacts the membranes and structures of the ear and nose, which then indirectly affect the throat.
Symptoms can include a perception of an increased sense of smell (for malodors), stuffiness, ear and nasal congestion, and a sore throat – which can occur every morning and evening for some women.
Some of these symptoms can last the entirety of pregnancy, but fortunately, they tend to resolve immediately after delivery.
Women should read further to learn why extra fluid impacts the ears, nose, and throat, and when to call an HCP, as some of these symptoms may require further assessment.
Background
Almost every aspect of the ear, nose, and throat (ENT) is affected during pregnancy, yet, these changes tend to be ignored or overlooked because their associated symptoms usually go away soon after delivery.
However, ENT changes during pregnancy can result in certain complications that can impact both a pregnant woman and her baby; therefore, they should always be discussed with an HCP.
Other than hormones, the largest, single factor during pregnancy that affects the ear, nose, and throat is fluid volume. The up to 6.5 liter increase in total body water throughout pregnancy affects all mucus membranes, leading to runny nose, stuffiness, congestion, and fluid in the nose and ears. Symptoms differ according to trimesters, but generally get worse as pregnancy progresses.
Nasal Changes
In non-pregnant individuals, rhinitis – the medical term for inflammation and swelling of the mucous membrane of the nose, characterized by a runny nose and/or stuffiness – is usually caused by the common cold or seasonal allergies.
Rhinitis during pregnancy is nasal congestion caused by a common cold or allergies while pregnant.
Gestational (or pregnancy) rhinitis is nasal congestion without a common cold or allergy, due to pregnancy-specific physiological changes in the nose.
Women can potentially experience both of these conditions during pregnancy, either at separate times or at the same time. While both conditions produce similar symptoms, treatment is very different.
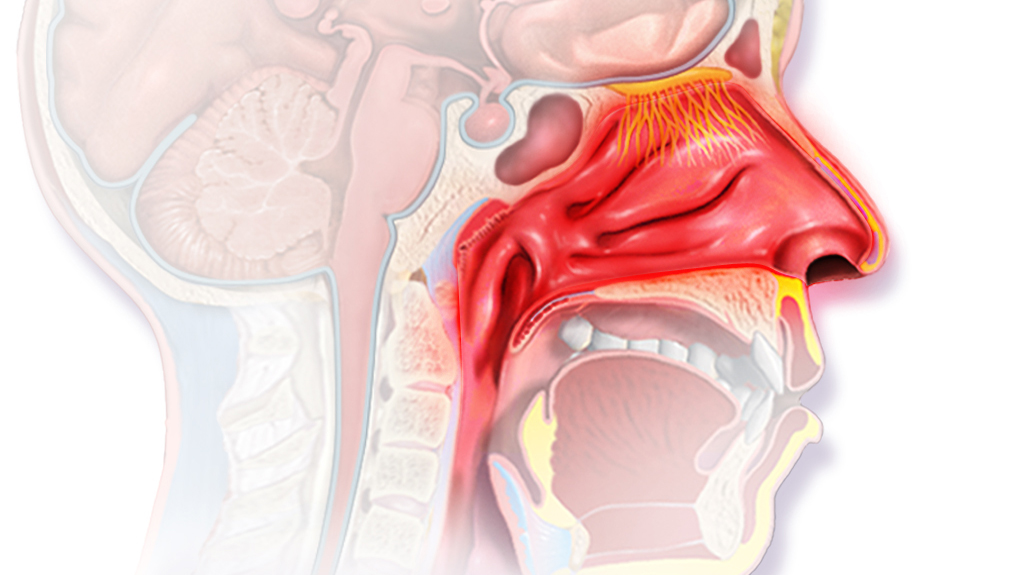
Nasal congestion can occur almost immediately in early pregnancy due to hormone and blood volume changes that increase and inflame the capillaries (blood vessels) in the nose. (Note: The cardiovascular system is one of the first organ systems affected in both mother and embryo).
Exactly how hormones affect nasal congestion/stuffiness and which hormones are responsible is not known.
Read more detailed information regarding nasal congestion during pregnancy and its management and treatment.
Sense of Smell
It does not appear that pregnancy-related changes influence a pregnant woman’s ability to smell – for better or for worse, despite its apparent prevalence.
It’s been documented for more than 100 years that pregnant women appear to have a heightened sense of smell – known as hyperosmia.
Women taking oral contraceptives, fertility treatments, and individuals on the HCG diet have also been reported to have a heightened sense of smell which would point to HCG as the likely cause.
Further, researchers have theorized that pregnant woman may have a better sense of smell to protect the developing embryo by reducing the likelihood that the mother will ingest toxins, similar to the protection hypothesis of Nausea and Vomiting of Pregnancy.
However – despite the above, science has been unable to confirm that pregnant women have a “better” sense of smell. Researchers have struggled to empirically explain this for the same 100 years.
Odor identification has been explored in pregnant women using a wide range of odors, with several methods, and in a number of different cultural contexts, with an overall lack of differences in sense of smell between pregnant and non-pregnant women.
There is no evidence that pregnant women generally identify odors consistently better than non-pregnant women, despite how common the symptom appears to be during pregnancy. In fact, some studies have even reported a tendency for worse odor identification in pregnancy, at least for some odors.
Further, in a study of 13,610 pregnant and 277,228 non-pregnant women who were part of the National Geographic Smell Study, pregnant women rated their own sense of smell significantly lower than non-pregnant women.
However, there is some slight evidence that pregnant women can identify some odors better than others and there may be an explanation. These items were identified as cooking odors, cigarette smoke, spoiled food, body odor, perfumes, spices, and coffee.
Given the overwhelming evidence that pregnant women, overall:
Do not have a better sense of smell than those who are not pregnant
Many pregnant women swearing the symptom is real
Evidence indicating pregnant women may notice certain unpleasant odors better than others
– indicates that pregnant women may simply be better aware of odors that are less pleasant or potentially harmful, and then pay more attention to them.
Bad smells attract more attention. The awareness that is drawn to these noxious odors may be incorrectly interpreted by pregnant women as a heightened sense of smell. When women are already aware that cigarette smoke, coffee, garbage, and spoiled food are associated with harm during pregnancy, these odors may become “stronger".
In one study that tested this theory, non-pregnant participants were exposed to an odor and were told it was a “natural, healthy extract” and it was rated as having a low intensity scent. After being told the same scent was “potentially hazardous”, those same participants rated it as having a high intensity scent.
These differences are also amplified when other individuals are not bothered by those scents and therefore do not notice them. This makes it appear as though pregnant have a better sense of smell, when in fact, they are likely subconsciously paying more attention to odors that may be harmful to their pregnancy.
However, women's experiences are different and science cannot always explain everything. Women are encouraged to submit their experience regarding their "sense of smell" during pregnancy at the bottom of this page.
Ear Changes
The inner ear has two functions: the cochlea is responsible for hearing, and the labyrinth for balance (detecting gravity and motion). Any alterations in these organs can cause major difficulties in any individual – not just pregnant women.
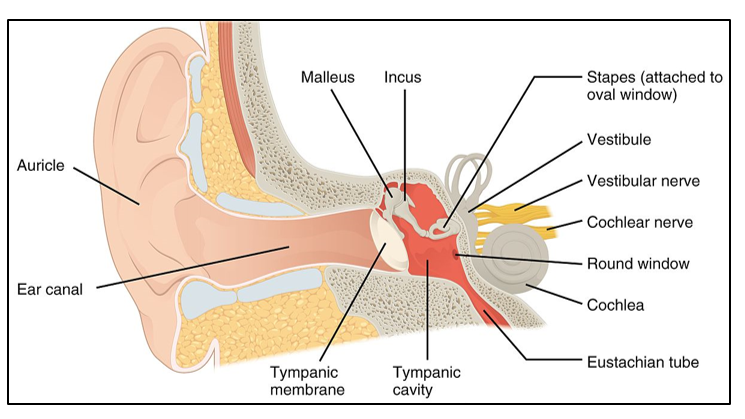
The eustachian tube connects the middle ear to the nose. Its purpose is to allow the air pressure in the middle ear to be equal to the air pressure in the environment, allowing the ear drum to vibrate freely.
Increased fluid volume during pregnancy that inflames nasal capillaries (described above) can block this tube (much like a common cold/allergies) and middle ear pressure cannot be balanced. Therefore, various symptoms result. It is likely that estrogen and progesterone may also play a role.
Pregnant women may feel dizzy, hear a ringing in the ears (tinnitus), experience a feeling of ear “fullness”, or lose the ability to hear clearly. Fortunately, all symptoms resolve after delivery, and in some cases – almost immediately.
Throat
Nasal congestion, heartburn/acid reflux, postnasal drip, and mouth-breathing (due to nasal congestion) – all increase during pregnancy and can cause a sore throat.
Women should inform their HCPs when they have a sore throat, especially repeated or severe, to rule out influenza, strep throat (group A streptococcus), snoring, acid reflux, mouth breathing, or sleep apnea.
Women should recognize that acid reflux can occur as early as the first trimester, without "heartburn". Reflux can cause chronic cough/sore throat as stomach acid irritates the lining of the back of the throat, especially during sleep. For some women, a sore throat (in the morning) may be the only symptom of early reflux (read more).
Action
Pregnant women should report all ENT symptoms to their HCP.
ENT physician: A medical specialist who is concerned with the diagnosis and treatment of disorders of the head and neck, particularly the ears, nose, and throat. Women may be referred to an ENT from their OB/GYN or midwife if their ENT-related symptoms during pregnancy are considered severe or very impactful to a woman's quality of life.
Nasal congestion can make pregnant women miserable, but can also be treated safely during pregnancy. Women should read nasal congestion to learn about possible management options (under the care of an HCP).
Women experiencing middle ear-type symptoms such as dizziness/fogginess should read more about Dizziness during pregnancy. Although this symptom is common, it is important to learn more to recognize and prevent any potential serious complications.
Gaps
Although hydration is a commonly recommended technique to relieve and "thin out" congestion/mucus in non-pregnant individuals, how effective is this during pregnancy?
Resources
ENT Health: videos, fact sheets (American Academy of Otolaryngology–Head and Neck Surgery Foundation)
Nasal Anatomy (University of California, Irvine)
Tinnitus and Pregnancy (British Tinnitus Foundation)